
Last reviewed: [January 2026]
How We Got Here: The GLP-1 Revolution
This miniature revolution has been driven by medications known as incretin analogues, or GLP-1 receptor agonists. It began in 2014 with liraglutide (brand name: Saxenda)1 but really took off in 2021 with the release of trial data showing that semaglutide (the famous Ozempic/Wegovy) produced around 14.9% average weight loss over 68 weeks, roughly doubling the efficacy of earlier treatments.2 The latest iteration, tirzepatide (Mounjaro/Zepbound), did better still, with an average 20.9% weight loss in trial patients over the same period.3
These are blockbuster drugs with blockbuster prices. In the UK, the cost of Mounjaro rose from around £189/month to £250–£300/month this summer, as the manufacturer (Eli Lilly) capitalised on extraordinary demand. And there’s more to come: there are at least six major next-generation incretin-based agents in late or mid-stage development.4 Retatrutide has earned the nickname “the Godzilla drug”, showing 24% weight loss at 48 weeks in phase-2 data.5 CagriSema, a combination of semaglutide and cagrilintide, has produced around 20% in phase-3 trials.6
New agents are also being designed to address current weaknesses. The two current leading drugs – semaglutide and tirzepatide – are weekly injections. One focus is on engineering injectables that can be given monthly instead. Also in the pipeline are oral agents, combinations designed to reduce side effects and to preserve muscle mass, which is vulnerable during periods of significant weight loss. Eli Lilly, for example, is testing semaglutide paired with bimagrumab, an antibody known to increase skeletal muscle.
What Stands Between a Breakthrough Drug and a UK Clinic
For a new obesity drug to become widely available in the UK, three things generally need to happen.
First, it must complete a large phase-3 programme confirming the phase-2 findings and ruling out major safety concerns.7
Second, the MHRA must review the data and grant a licence — a process that typically takes 9–12 months after phase-3 results.8-9 Once this licence is granted, the drug can usually be prescribed privately.
The third step is what determines wide NHS availability: appraisal by NICE, which assesses cost-effectiveness, negotiates pricing arrangements and defines the eligible patient groups.10-11 Even when NICE works in parallel with regulators, this process adds further months12, and the NHS still needs time to organise supply and capacity. Wegovy, for example, was authorised long before it became usable in practice because global demand outstripped supply.13,14,15,16
This means that a drug completing phase-3 trials today might reach private clinics in around a year, and the NHS in two to three years. Faster is possible, but uncommon; slower is common.
When the Process Goes Wrong: A Troubled History of Weight-Loss Drugs
And that assumes that everything goes to plan: the history of weight-loss science is littered with cautionary tales. The earliest effective weight-loss medication was 2,4-dinitrophenol (DNP). Originally an intermediate in the production of explosives, its medical significance became apparent in the 1930s when munitions workers exposed to it began losing weight at an alarming rate.17
DNP worked as a “mitochondrial uncoupler”18 — it disconnected the central metabolic pathways in cells, so that the fuel-burning processes were no longer harnessed to the production of usable energy but instead burned through glucose and oxygen at an unbridled rate. Some unfortunate patients were effectively consumed in the fire of their own rampant metabolism, suffering hyperthermia, dehydration and multi-organ failure. After a number of deaths, the drug was banned in 1938.19
A similar story unfolded in the 1990s with Fenfluramine-Phentermine (“Fen-Phen”). Young patients began presenting with breathlessness and heart murmurs, later found to be signs of scarred heart valves and structural changes in the major blood vessels supplying the lungs (resulting in ‘pulmonary hypertension’), both unintended consequences of activating a subset (‘5-HT₂B’)20 of serotonin receptors. Fen-Phen was withdrawn in 1997.21
The result is that obesity drugs face an even more rigorous licensing process than other drugs: they have to demonstrate both psychiatric and cardiovascular safety before they will be accepted by regulators such as the FDA and MHRA/EMA.
In total, more than a dozen anti-obesity drugs have been withdrawn, restricted, or abandoned due to safety concerns22,23, the most recent of which was danuglipron, a promising oral GLP-1 from Pfizer that might otherwise have reached the market by 2025.24
A Realistic UK Timeline
So any predictions about when we’re likely to see these drugs in the UK are subject to some significant caveats and assumptions, but assuming successful trial results continue and there is a typical regulatory review period, a rough timeline might look like this. The earliest of these drugs could become available in the UK in early 2026, following the FDA approval of high-dose oral semaglutide in December 2025, assuming no unanticipated regulatory or supply impediments.
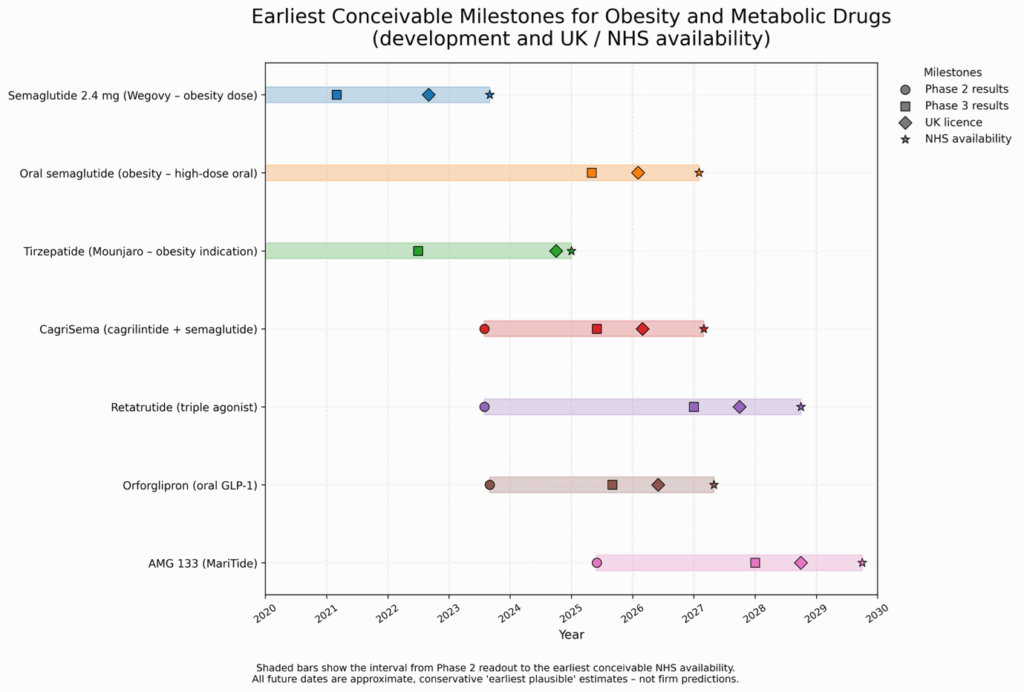
Figure references: 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35
The Impact on UK Practise
A jump from 20% average weight loss (tirzepatide, in trial data) to 24% weight loss (with retatrutide, again in trials) will make a difference to some very obese patients.36 That’s very exciting, but potency isn’t what’s missing in the treatments we already have.
The drug which we seem most likely to see next is oral semaglutide (the oral version of Ozempic/Wegovy). A weekly medication might be expected to improve adherence simply because there are fewer opportunities to forget. But injectables bring their own frictions. The availability of an oral option will probably have its biggest impact on uptake – overcoming an obstacle for some patients. But it may improve consistency too: in my own practice, a noticeable minority of patients delay injections, struggle with technique, or occasionally miss a dose.
This matters because, at least early in treatment, the effect of the drugs is strongest in the days after a dose; towards the end of each week, my patients report a return of cravings and appetite – a weakening of the control that these medications rely on for their effect. Weight-loss clinicians have long been familiar with the potential impact of even a short interruption of dietary control: each kilogram of body fat loss is achieved with a hard-fought ~7,700-calorie deficit.37 For people biologically inclined to enjoy food, that deficit is easily whittled away by a few days of normal or uninhibited eating. Even short interruptions in treatment can make all the difference.
In that respect, an oral agent, even with the same side-effect profile, may improve outcomes for some patients. The more significant cause of treatment interruption, however, is the gastrointestinal side effects – nausea, vomiting, diarrhoea, constipation.38 It’s not clear that oral semaglutide will do much to solve this problem. The hope is that agents which rely less on GLP-1 mimicry – like Cagri Sema, and MariTide – may address this concern, but this is yet to be borne out decisively in data.
But the factor with the biggest real-world impact is cost. Again, many of my patients have had periods of interruption to their weight-loss treatment which have been down to cost — they’ve been unable to afford, or bring themselves to spend, the £250+ cost of their monthly Mounjaro. Treatment interruptions are a significant reason for the gap between the astonishing average weight loss achieved in trials and the real-world data.39,40
The steep prices of these agents are also the major reason why they are not in wider use – on the private market, because most people simply can’t afford treatment costing £300 per month, and, on the NHS, where funding is limited by national edict to only the most severe cases.
A Complex Drug is a Costly Drug
Current injectables require refrigeration.41 If a Mounjaro pen is removed from the fridge, it must be used within 30 days.42 Since a pen needs to last the patient four weeks, any breach of the cold chain from manufacturer to pharmacy makes the pen unsellable. This drives up costs for manufacturers, distributors and suppliers as well as being a headache for patients.
Of great interest from this perspective is orforglipron, a competing agent slightly further back in the pipeline. GLP-1, the molecule in the human body which all the current leading drugs mimic, is a peptide — a chain of amino acids.43 Peptides are large, complex and delicate molecules with correspondingly complex manufacturing processes that scale slowly and at great cost.44 In contrast, orforglipron is a small molecule, made via standard organic synthesis, with simpler manufacturing processes that are less expensive to scale.45,46
Cost is Not Price
In that sense, I’m most excited by anything that will drive down the price. Simpler manufacturing and the absence of a cold chain are helpful (they lower the theoretical price floor) but they are not sufficient. Oral semaglutide is already available for diabetes (branded Rybelsus) and its cost is much the same as the injectable version.47 This is consistent with what’s known about pharmaceutical pricing. What seems to drive prices at the moment is not so much manufacturing or transport costs as intense demand and the desire of the pharmaceutical companies (Eli Lilly, and Novo Nordisk) to recoup their R&D costs and realise their profits while their patents last.48,49,50
So, what I’m most enthusiastic about is competition. In countries like India and China the patents start expiring as early as 2026–2028.51 In the UK, however, patents for semaglutide and tirzepatide run well into the early 2030s. So, for competition, we will need to look to new entrants. But who are the developers of the next four drugs in the pipeline? Novo Nordisk and Eli Lilly.
Frequently Asked Questions
These answers provide a general overview. For detailed explanations, evidence summaries, and treatment comparisons, see our in-depth guides in the Knowledge Hub.